
Bovine Respiratory Disease
|
Bovine Respiratory Disease (BRD), sometimes described as "shipping fever,” is the most common and costly disease affecting the North American beef cattle industry. In the broadest sense, BRD refers to any disease of the upper or lower respiratory tracts. Although commonly associated with the feedlot, BRD can also be a significant problem in cow-calf herds. Several BRD pathogens can also cause abortions in pregnant cows, and BRD is a leading cause of illness, antibiotic treatment and death in nursing calves between three weeks of age and weaning. BRD can be much more difficult to detect and effectively treat in cows and calves on pasture compared to cattle in confined facilities. Delayed BRD diagnosis and treatment increases the risk of secondary bacterial infections, severe illness and death. |
|
Sections
Key Points
|
Causes
BRD is a complex disease involving several interacting factors. For example, researchers can recover many of the bacteria and viruses responsible for BRD from the nasal passages of healthy cattle. However, other factors such as the stresses from transportation, mixing unfamiliar cattle and adverse weather create the right mix of circumstances for BRD to develop. There are three main categories of factors associated with all diseases, and BRD in particular:
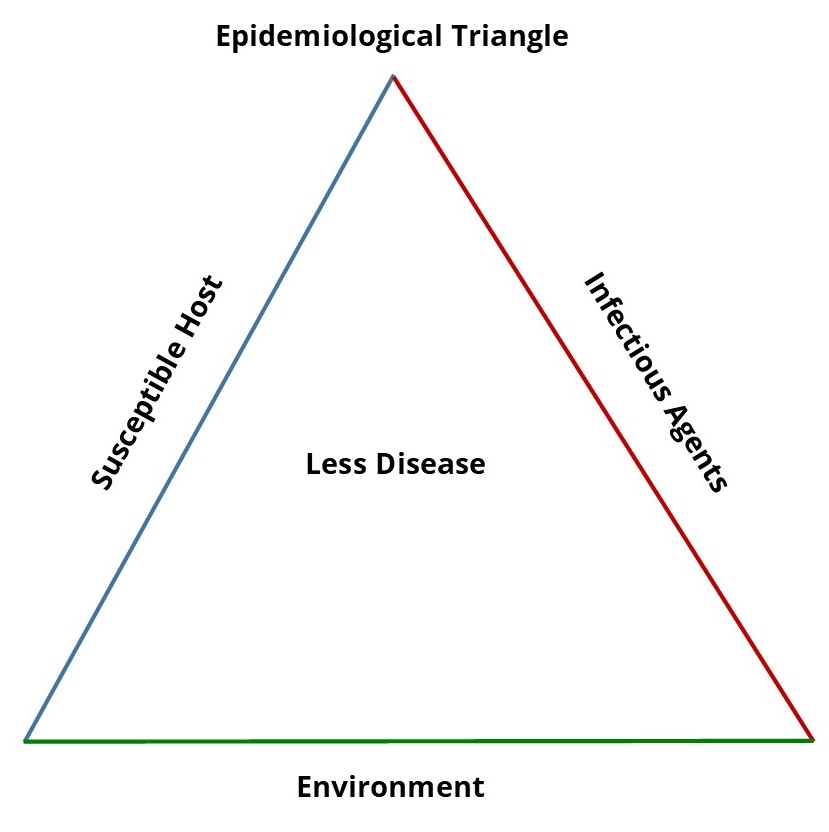
- Host factors, which refers to the characteristics of an animal that make it more prone to the disease, such as: age, nutritional status, immune status, prior exposure to the pathogens, genetics (e.g., crossbreds generally have better health performance than straightbred cattle)
- Infectious agents or pathogens must be present to cause the disease. These can broadly be categorized as viruses, bacteria and parasites:
- Viruses, including bovine herpes virus (IBR), bovine parainfluenza virus (PI-3), bovine respiratory syncytial virus (BRSV), bovine viral diarrhea virus (BVD) and bovine coronavirus (BCV). These viruses usually cause the initial BRD infection and predispose the animal to subsequent bacterial BRD infections. Several of these viruses can also cause significant reproductive (BVD, IBR) or diarrhea (BVD, BCV) challenges in cow-calf operations.
- Bacteria, including Mannheimia haemolytica, Pasteurella multocida, Histophilus somni and Mycoplasma bovis.
- Parasites, including lungworm.
- The environment that the animal is in may increase the risk factors for disease. Animals in overcrowded conditions, in poor air quality (poor ventilation, dust, smoke), sourced from auction markets or stressed by transport, commingling, temperature fluctuations, etc. are more likely to develop the disease.
This interview with veterinarian Dr. Steve Hendrick, DVM, by RealAgriculture.com explains how to recognize and deal with cattle with respiratory disease.The next video begins with an excellent explanation of BRD. It is included for information purposes only and does not constitute or imply an endorsement, recommendation or favoring by the BCRC or the CCA.
Clinical Signs
Abortion may be an easily-overlooked sign that BRD pathogens are circulating in the cow herd. The viruses that cause IBR and BVD can cause abortion in unvaccinated females.
The BVD virus can suppress immunity and lead to a variety of infectious diseases in young calves.
BRD pathogens cause respiratory disease in calves prior to weaning. Clinical signs of BRD in pre-weaned calves, feedlot calves and grass cattle include:
- fever of over 40°C (>104°F)
- difficulty breathing occurred to varying degrees
- nasal discharge
- varying degrees of depression
- diminished or no appetite ("off feed")
- rapid, shallow breathing
- coughing
BRD is the most common disease of feedlot cattle, with peak incidence (often associated with Mannheimia haemolytica) generally occurring within two weeks of arrival. Generally, cattle exhibiting signs of depression separate themselves from the rest of the herd, and diligent pen checkers will usually identify most sick animals. Body temperature is commonly used to determine whether cattle should be treated. Body temperature is such an important diagnostic test that many feedlots will treat animals based upon an undifferentiated fever (UF).
BRD can also occur 30-40 days after arrival, after the stock attendants have reduced their level of surveillance of newly arrived animals. These BRD cases are more likely to involve Mycoplasma bovis, and their clinical signs can be more difficult to detect. Cattle with Mycoplasma pneumonia may not appear depressed, but instead demonstrate a chronic cough and weight loss. Mycoplasma can also infect joints and result in a profound lameness, reluctance to move, poor appetite and a poor or prolonged response to treatment.
Risk factors
BRD is considered a polymicrobial disease, which means that it arises from infections with a combination of bacteria and viruses. In addition, several other factors influence the susceptibility of an animal to developing BRD. Any one risk factor alone may not trigger BRD, but several risk factors together form an additive effect that can predispose the animal to BRD.
Management factors have been associated with BRD for decades. Regardless of herd size, outbreaks of BRD (20% of herds) were most common in herds that had purchased 10 or more bulls, used community pastures, bought cows or did not vaccinate newly purchased animals.3 Historically, feeder cattle were often shipped by train, particularly to large markets in the United States. It was recognized at the time that shipping was a risk factor for BRD, and hence pneumonia in cattle was termed “shipping fever.” A study involving calves arriving at 21 U.S. commercial feedlots from 1997 to 2009 concluded that distance traveled was correlated to the incidence of BRD.4 This, however, has not been substantiated in Canada.
Weather has always been implicated in the occurrence of BRD, presumably because the greatest incidence of BRD occurs during the fall. However, this is confounded by the fact that it is also when the greatest number of calves is being assembled, mixed (commingled) and transported. A study involving 288,388 head of cattle, arriving at nine U.S. commercial feedlots during September to November in 2005 to 2007, found that wind chill and temperature change were associated with an increased incidence of BRD.5
Some studies have found a higher incidence of BRD in auction market versus ranch-derived calves. Furthermore, the incidence of BRD increases with the level of commingling; calves assembled from multiple lots are more likely to have BRD than pens composed of larger groups of calves from fewer sources. There is also considerable anecdotal evidence that the quality of the calves purchased is highly associated with the incidence of BRD, with poorer quality calves (e.g., lightweight, malnourished, uncastrated, unvaccinated) having more BRD. Studies also conclude that lighter weight calves have a higher risk of developing BRD than do their heavier pen mates.
It is unclear whether heifers are more prone to developing BRD than steers. A large-scale U.S. study involving 21 million animals found that heifers were at a greater risk of developing BRD than were males from 1997-1999, but no difference in between steers and heifers was found during 1994-1996.6
Rapid introduction to high-grain rations may also precipitate cases of BRD.
The risk factors associated with an outbreak in one feedlot may not be the same as outbreaks at other feedlots involving similar types of animals in similar conditions.
Prevention
Disease prevention in the cow-calf herd
Vaccination: Work with your veterinarian to develop and implement a prevention-based herd health management program for both the breeding herd and calf crop. They will be able to recommend a vaccination program that is appropriate for your herd, your management system and your marketing practices.
Biosecurity: Your veterinarian can also help you develop an effective biosecurity program to reduce the risk that new diseases will be introduced when new bulls or replacement females are introduced to the herd.
Colostrum: The first few hours of the calf's life are critical to determining whether it survives to weaning and beyond. Without colostrum, the newborn calf's immature immune system can't adequately protect it against diseases like scours. But enough colostrum of adequate quality will give the calf a good start in life that pays health dividends through weaning.
Nutrition: Test your feed and work with a nutritionist to correct any deficiencies or imbalances. Good feed supports good health, and good overall health is key to combatting BRD pathogens. Cows in good body condition score (BCS) also produce more and higher-quality colostrum.
Stress: Stress depresses the immune system, makes it harder for the animal to fight off pathogens or take full advantage of protective vaccines. It's impossible to eliminate stress, but castrating, dehorning, branding (if necessary) and vaccinating early in life takes some of the stress off at weaning/processing time in the fall, which is a stressful time already. Low-stress weaning practices (like two-stage, fenceline weaning) can improve feed intake and reduce the need for BRD treatments.
Crowding: Cattle are more likely to transmit BRD pathogens when they are in close contact. Transportation, regular handling and sorting (e.g., during processing) and intensive grazing practices may increase the risk of disease spread.7
The health benefits of these practices are not restricted to BRD. They help reduce the risk of most, if not all diseases caused by viruses, bacteria or parasites.
|
Preconditioning appears to have some benefit in preventing BRD, with weaning four to six weeks before sale being the most important component of a preconditioning program. The concept of preconditioning calves to decrease stress levels was first introduced in 1967. While there is considerable variation in what constitutes a preconditioning program, the central components entail:
|
|
After calves arrive at the feedlot
Vaccines for respiratory diseases are routinely administered upon arrival at the feedlot, which may also be a difficult time for a stressed calf to mount an effective immune response. A recent review of the scientific literature found no clear benefit from vaccinating calves upon arrival at the feedlot.8 Another review relating to Mannheimia haemolytica, Pasteurella multocida, and Histophilus somni vaccines concluded that there was a potential benefit for vaccinating feedlot cattle against M. haemolytica and P. multocida but not H. somni.9
Nutrition may affect incidence of BRD. One review found that increased energy density (concentrates) will improve ADG without adversely affecting the incidence of BRD.10 Other studies found that the incidence of BRD tended to increase once concentrates exceeded 50% of the diet.11 Similarly, BRD morbidity increased once crude protein exceeded 14%. There is not enough evidence to conclude that injected doses of vitamins A, D and E will reduce BRD. A wide range of studies have also examined supplementing with potassium, thiamine, B-vitamins, copper, zinc, vitamin E, selenium and bypass protein. Although these studies haven't shown that supplementing with these nutrients significantly reduce the incidence of BRD, it's likely that significant deficiencies of these nutrients would almost certainly impair animal health.
Metaphylactic treatment strategies using injectable antibiotics can help control BRD in high-risk calves, and likely are more effective than oral antibiotics since stressed cattle may not be eating or drinking regularly.12 It is important that producers consult with their veterinarian regarding the use of antibiotics for the control and treatment of BRD, especially in terms of avoiding antibiotic resistance.
Good animal husbandry can also help reduce the risk of disease. Providing clean, dry bedding, protection from prevailing winds, avoiding overcrowding, using low-stress handling techniques, proper ventilation of barns and minimizing dust can help to reduce disease.
Treatment
There is a large body of scientific knowledge regarding the beneficial effects of antibiotics for treating BRD. The question is not whether to treat an animal diagnosed with BRD with an antibiotic, but rather, "which antimicrobial works best?” There is no simple answer to this latter question, but your veterinarian is a good place to start.
Ancillary drugs, such as nonsteroidal anti-inflammatories (NSAIDS) and immunomodulators, have been used to treat BRD for decades. However, many of the studies have been small-scale experiments and there is a lack of data from well-designed, large-scale, clinical trials. However, a 2011 study found that meloxicam (NSAID) administered in water 24 hours before castration at the feedlot significantly reduced the number of animals that developed BRD.14
Even when working with the best recommendations, sometimes treatments fail. Common causes of treatment failure include:
- Disease too far advanced (due to delayed detection and treatment)
- Wrong diagnosis (e.g., calves are sick with a nutritional disease like grain overload)
- Viral infections with no bacterial involvement
- Simultaneous disease process (e.g., overt IBR in feedlot calves, post-calving metritis in cows)
- Inappropriate antibiotic used (i.e., the organism is resistant to the antibiotic chosen)
- Overuse or inappropriate use of ancillary drugs like anti-inflammatory and immunomodulator drugs
Doing necropsies on sick animals early in an outbreak can help to diagnose and treat the problem more quickly and accurately, potentially allowing time to develop protocols to deal with the disease more appropriately.
Carcass Quality Considerations
Current Research
Research into BRD is happening on numerous fronts. Current research is looking at further understanding the respiratory microbiome and the differences in the microbiome between healthy and sick cattle. Current research is also examining antibiotic resistance, improved diagnostics, more reliable and effective non-antibiotic therapies, better vaccines and a more solid understanding of the disease complexes.
Feedback
Feedback and questions on the content of this page are welcome. Please e-mail us at info@beefresearch.ca.
Acknowledgements
Thanks to:
- Dr. John Campbell, Professor, Department of Large Animal Clinical Sciences, University of Saskatchewan
- Dr. Murray Jelinski, Professor and Alberta Chair in Beef Cattle Health and Production Medicine at the Western College of Veterinary Medicine, University of Saskatchewan
for contributing their time and expertise to writing this page.
This topic was last revised on November 26, 2021 at 2:40 AM.
Related Topics
Related Blog Posts
- November 23, 2021: Always Look a Gift Cow in the Mouth
- October 25, 2021: Basics of Backgrounding - Veterinary & Expert Insights Across Canada Webinar November 17th
- October 8, 2021: Is This a Good Investment?
- April 29, 2021: “Beefed up” methods to study prebiotics
- February 18, 2021: Protecting Your Investment: Bull Management
- January 7, 2021: What’s been done and what’s next? An update from our Executive Director, Andrea Brocklebank
- December 30, 2020: Top 10 Articles of 2020
- October 13, 2020: Everything Old is New Again – Treating Chronic Mycoplasma
- March 31, 2020: Think you have a closed herd? Think again.
- March 24, 2020: The Cost Benefit of Using Vaccines in Beef Cattle
- December 30, 2019: Top 10 Blog Posts of 2019
- October 10, 2019: The cost-benefit of using vaccines: bovine respiratory disease
- September 26, 2019: The Cost Benefit of Using Vaccines: BVD
- August 29, 2019: How to get new feedlot calves settled and gaining quickly; advice from producers, veterinarians and feedlot consultants
- October 29, 2018: Antibiotic Use in Canadian Feedlots
- October 5, 2018: Developing Faster, Less Expensive Diagnostic Tests
- September 18, 2017: Bovine Respiratory Disease from the Farm to the Feedlot
- November 10, 2016: Results of the Beef Research Priority Survey
- November 1, 2016: Antibiotic Alternatives
- September 15, 2016: 5 ways cattle feeders can prepare for the fall run
Fact Sheets
-
In Progress.
Results expected in March 2022.
Antibiotic resistance in bovine respiratory disease bacteria
 View Web Page
View Web Page
 View PDF
View PDF
-
March 2021
Can chute-side disease diagnostics reduce antibiotic use in beef cattle?
View Web Page
View PDF
-
March 2020
Can prebiotics and probiotics help avoid respiratory disease and antimicrobial treatment in beef cattle?
View Web Page
View PDF
-
In Progress.
Results expected in April 2022.
Develop a faster thermometer for use in cattle
View Web Page
View PDF
-
2016
Developing efficient, multi-pathogen tests for common cattle diseases
View Web Page
View PDF
-
In Progress.
Results expected in 2023.
Developing more rapid, accurate and cost-effectiveness BRD diagnostics
View Web Page
View PDF
-
In Progress.
Results expected in March 2022.
Do transportation and rest stops affect lung health?
View Web Page
View PDF
-
March 2018
Establishing a long term surveillance network to support Canadian beef cattle research
View Web Page
View PDF
-
In Progress.
Results expected in March 2022.
Exploring non-antibiotic treatment options for BRD
View Web Page
View PDF
-
August 2010
How Mycoplasma Spreads
View Web Page
View PDF
-
April 2014
Improving Calf Transportation
View Web Page
View PDF
-
September 2009
Managing Mycoplasma
View Web Page
View PDF
-
August 2006
Preventing Shipping Fever Pneumonia in Calves
View Web Page
View PDF
-
June 2007
Seeking More Effective Treatment for an Economically Important Disease
View Web Page
View PDF
-
August 2004
Seeking to Prevent Deaths of Feedlot Calves
View Web Page
View PDF
-
In Progress.
Results expected in March 2022.
Understanding Mycoplasma bovis
View Web Page
View PDF
-
In Progress.
Results expected in March 2021.
Understanding Mycoplasma bovis pneumonia in beef cattle
View Web Page
View PDF
-
In Progress.
Results expected in August 2022.
Vaccination programs to improve calf health
View Web Page
View PDF
-
August 2004
Vaccine improvement could decrease agricultural use of antibiotics
View Web Page
View PDF
-
In Progress.
Results expected in May 2021.
What can we learn from good feedlot pen checkers?
View Web Page
View PDF
-
March 2011
Improved BVD Vaccine
by Alberta Beef Producers
View Web Page
View PDF
-
October 2008
Improved Prevention and Management of Bovine Respiratory Disease
by Alberta Beef Producers
View Web Page
View PDF
-
March 2010
Mycoplasma Strains
by Alberta Beef Producers
View Web Page
View PDF
-
2019
New Diagnostics to Inform Antimicrobial Treatment Decisions
by Alberta Beef Producers
View Web Page
View PDF
-
March 2013
Studying unusual feedlot mortalities
by Alberta Beef Producers
View Web Page
View PDF
-
May 2015
Testing for antimicrobial resistance in the field
by Alberta Beef Producers
View Web Page
View PDF
-
December 2010
Trying to Prevent Mycoplasma
by Alberta Beef Producers
View Web Page
View PDF